This piece is based on my talk to the UCL conference ‘The Role of Diagnosis in Clinical Psychology’. It was aimed at an audience of clinical psychologists but should be of interest more widely.
I’ve been a long–term critic of psychiatric diagnoses but I’ve become increasingly frustrated by the myths and over-generalisations that get repeated and recycled in the diagnosis debate.
So, in this post, I want to tackle some of these before going on to suggest how we can critique diagnosis more effectively. I’m going to be referencing the DSM-5 but the examples I mention apply more widely.
“There are no biological tests for psychiatric diagnoses”
“The failure of decades of basic science research to reveal any specific biological or psychological marker that identifies a psychiatric diagnosis is well recognised” wrote Sami Timini in the International Journal of Clinical and Health Psychology. “Scientists have not identified a biological cause of, or even a reliable biomarker for, any mental disorder” claimed Brett Deacon in Clinical Psychology Review. “Indeed”, he continued “not one biological test appears as a diagnostic criterion in the current DSM-IV-TR or in the proposed criteria sets for the forthcoming DSM-5”. Jay Watts writing in The Guardian states that “These categories cannot be verified with objective tests”.
Actually there are very few DSM diagnoses for which biological tests are entirely irrelevant. Most use medical tests for differential diagnosis (excluding other causes), some DSM diagnoses require them as one of a number of criteria, and a handful are entirely based on biological tests. You can see this for yourself if you take the radical scientific step of opening the DSM-5 and reading what it actually says.
There are some DSM diagnoses (the minority) for which biological tests are entirely irrelevant. Body dysmorphic disorder (p242), for example, a diagnosis that describes where people become overwhelmed with the idea that a part of their body is misshapen or unattractive, is purely based on reported experiences and behaviour. No other criteria are required or relevant.
For most common DSM diagnoses, biological tests are relevant but for the purpose of excluding other causes. For example, in many DSM diagnoses there is a general exclusion that the symptoms must be not attributable to the physiological effects of a substance or another medical condition (this appears in schizophrenia, OCD, generalized anxiety disorder and many many others). On occasion, very specific biological tests are mentioned. For example, to make a confident diagnosis of panic disorder (p208), the DSM-5 recommends testing serum calcium levels to exclude hyperparathyroidism – which can produce similar symptoms.
Additionally, there are a range of DSM diagnoses for which biomedical tests make up one or more of the formally listed criteria but aren’t essential to make the diagnosis. The DSM diagnosis of narcolepsy (p372) is one example, which has two such criteria: “Hypocretin deficiency, as measured by cerebrospinal fluid (CSF) hypocretin-1 immunoreactivity values of one-third or less of those obtained in healthy subjects using the same assay, or 110 pg/mL or less” and polysomnography showing REM sleep latency of 15 minutes or less. Several other diagnoses work along these lines – where a biomedical tests results are listed but are not necessary to make the diagnosis: the substance/medication-induced mental disorders, delirium, neuroleptic malignant syndrome, neurocognitive disorders, and so on.
There are also a range of DSM diagnoses that are not solely based on biomedical tests but for which positive test results are necessary for the diagnosis. Anorexia nervosa (p338) is the most obvious, which requires the person to have a BMI of less than 17, but this applies to various sleep disorders (e.g. REM sleep disorder which requires a positive polysomnography or actigraphy finding) and some disorders due to other medical conditions. For example, neurocognitive disorder due to prion disease (p634) requires a brain scan or blood test.
There are some DSM diagnoses which are based exclusively on biological test results. These are a number of sleep disorders (obstructive sleep apnea hypopnea, central sleep apnea and sleep-related hypoventilation, all diagnosed with polysomnography).
“Psychiatric diagnoses ‘label distress'”
The DSM, wrote Peter Kinderman and colleagues in Evidence-Based Mental Health is a “franchise for the classification and diagnosis of human distress”. The “ICD is based on exactly the same principles as the DSM” argued Lucy Johnstone, “Both systems are about describing people’s distress in terms of medical diagnosis”
In reality, some psychiatric diagnoses do classify distress, some don’t.
Here is a common criterion in many DSM diagnoses: “The symptoms cause clinical significant distress or impairment in social, occupational or other important areas of functioning”
The theory behind this is that some experiences or behaviours are not considered of medical interest unless they cause you problems, which is defined as distress or impairment. Note however, that it is one or the other. It is still possible to be diagnosed if you’re not distressed but still find these experiences or behaviours get in the way of everyday life.
However, there are a whole range of DSM diagnoses for which distress plays no part in making the diagnosis.
Here is a non-exhaustive list: Schizophrenia, Tic Disorders, Delusional Disorder, Developmental Coordination Disorder, Brief Psychotic Disorder, Schizophreniform Disorder, Manic Episode, Hypomanic Episode, Schizoid Personality Disorder, Antisocial Personality Disorder, and so on. There are many more.
Does the DSM ‘label distress’? Sometimes. Do all psychiatric diagnoses? No they don’t.
“Psychiatric diagnoses are not reliable”
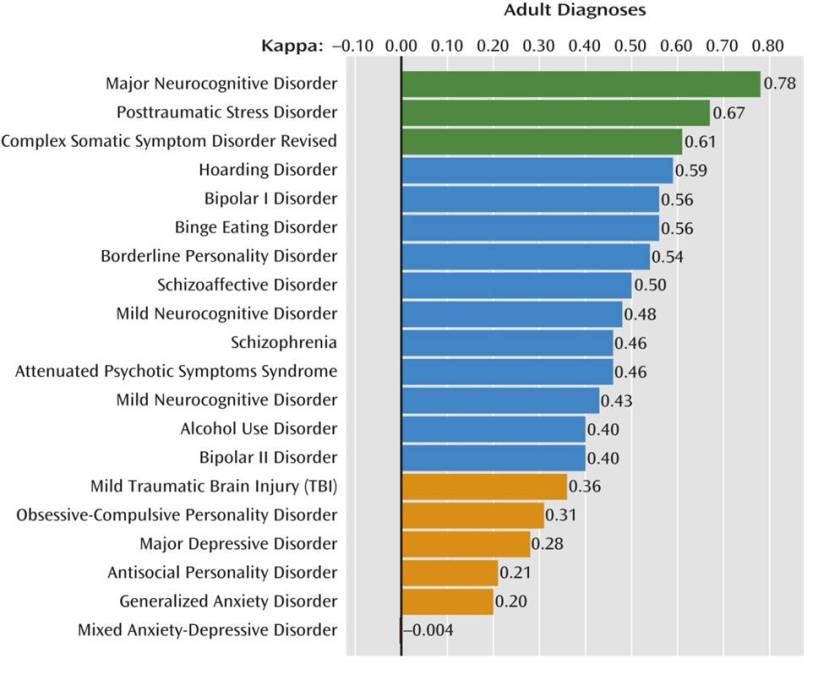
The graph below shows the inter-rater reliability results from the DSM-5 field trial study. They use a statistical test called Cohen’s Kappa to test how well two independent psychiatrists, assessing the same individual through an open interview, agree on a particular diagnosis. A score above 0.8 is usually considered gold standard, they rate anything above 0.6 in the acceptable range.
The results are atrocious. This graph is often touted as evidence that psychiatric diagnoses can’t be made reliably.
However, here are the results from a study that tested diagnostic agreement on a range of DSM-5 diagnoses when psychiatrists used a structured interview assessment. Look down the ‘κ’ column for the reliability results. Suddenly they are much better and are all within the acceptable to excellent range.
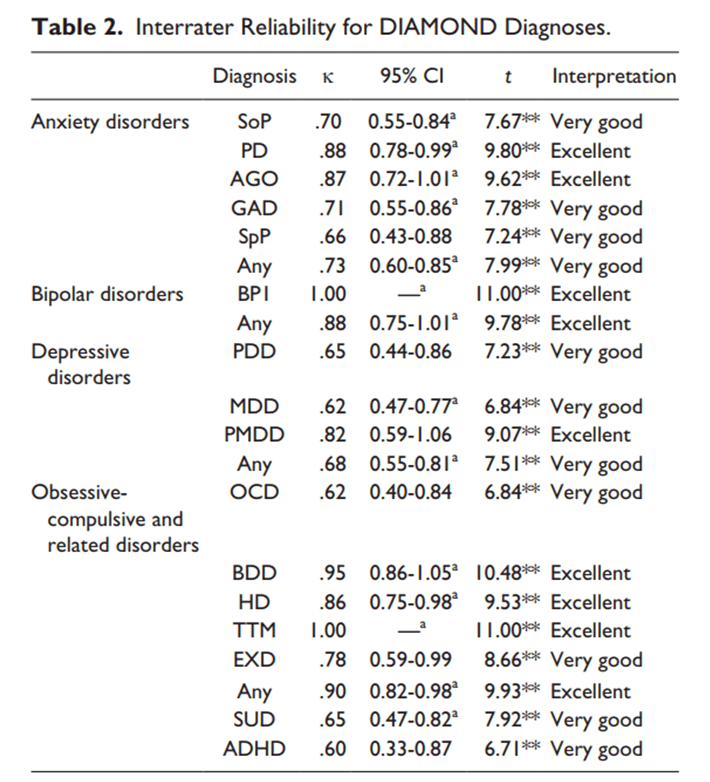
This is well-known in mental health and medicine as a whole. If you want consistency, you have to use a structured assessment method.
While we’re here, let’s tackle an implicit assumption that underlies many of these critiques: supposedly, psychiatric diagnoses are fuzzy and unreliable, whereas the rest of medicine makes cut-and-dry diagnoses based on unequivocal medical test results.
This is a myth based on ignorance about how medical diagnoses are made – almost all involve human judgement. Just look at the between-doctor agreement results for some diagnoses in the rest of medicine (which include the use of biomedical tests):
Diagnosis of infection at the site of surgery (0.44), features of spinal tumours (0.19 – 0.59), bone fractures in children (0.71), rectal bleeding (0.42), paediatric stroke (0.61), osteoarthritis in the hand (0.60 – 0.82). There are many more examples in the medical literature which you can see for yourself.
The reliability of DSM-5 diagnoses is typically poor for ‘off the top of the head’ diagnosis but this can be markedly improved by using a formal diagnostic assessment. This doesn’t seem to be any different from the rest of medicine.
“Psychiatric diagnoses are not valid because they are decided by a committee”
I’m sorry to break it to you, but all medical diagnoses are decided by committee.
These committees shift the boundaries, revise, reject and resurrect diagnoses across medicine. The European Society of Cardiology revise the diagnostic criteria for heart failure and related problems on a yearly basis. The International League Against Epilepsy revise their diagnoses of different epilepsies frequently – they just published their revised manual earlier this year. In 2014 they broadened the diagnostic criteria for epilepsy meaning more people are now classified as having epilepsy. Nothing changed in people’s brains, they just made a group decision.
In fact, if you look at the medical literature, it’s abuzz with committees deciding, revising and rejecting diagnostic criteria for medical problems across the board.
Humans are not cut-and-dry. Neither are most illnesses, diseases and injuries, and decisions about what a particular diagnosis should include is always a trade-off between measurement accuracy, suffering, outcome, and the potential benefits of intervention. This gets revised by a committee who examine the best evidence and come to a consensus on what should count as a medically-relevant problem.
These committees aren’t perfect. They sometimes suffer from fads and group think, and pharmaceutical industry conflicts of interest are a constant concern, but the fact that a committee decides a diagnosis does not make it invalid. I would argue that psychiatry is more prone to fads and pressure from pharmaceutical company interests than some other areas of medicine although it’s probably not the worst (surgery is notoriously bad in this regard). However, having a diagnosis decided by committee doesn’t make it invalid. Actually, on balance, it’s probably the least worst way of doing it.
“Psychiatric diagnoses are not valid because they’re based on experience, behaviour or value judgements”
We’ve discussed above how DSM diagnoses rely on medical tests to varying degrees. But the flip side of this, is that there are many non-psychiatric diagnoses which are also only based on classifying experience and/or behaviour. If you think this makes a diagnosis invalid or ‘not a real illness’ I look forward to your forthcoming campaigning to remove the diagnoses of tinnitus, sensory loss, many pain syndromes, headache, vertigo and the primary dystonias, for example.
To complicate things further, we know some diseases have a clear basis in terms of tissue damage but the diagnosis is purely based on experience and/or behaviour. The diagnosis of Parkinson’s disease, for example, is made this way and there are no biomedical tests that confirm the condition, despite the fact that studies have shown it occurs due to a breakdown of dopamine neurons in the nigrostriatal pathway of the brain.
At this point, someone usually says “but no one doubts that HIV or tuberculosis are diseases, whereas psychiatric diagnosis involves arbitrary decisions about what is considered pathological”. Cranks aside, the first part is true. It’s widely accepted – rightly so – that HIV and tuberculosis are diseases. However, it’s interesting how many critics of psychiatric diagnosis seem to have infectious diseases as their comparison for what constitutes a ‘genuine medical condition’ when infectious diseases are only a small minority of the diagnoses in medicine.
Even here though, subjectivity still plays a part. Rather than focusing on a single viral or bacterial infection, think of all viruses and bacteria. Now ask, which should be classified as diseases? This is not as cut-and-dry as you might think because humans are awash with viruses and bacteria, some helpful, some unhelpful, some irrelevant to our well-being. Ed Yong’s book I Contain Multitudes is brilliant on this if you want to know more about the massive complexity of our microbiome and how it relates to our well-being.
So the question for infectious disease experts is at what point does an unhelpful virus or bacteria become a disease? This involves making judgements about what should be considered a ‘negative effect’. Some are easy calls to make – mortality statistics are a fairly good yardstick. No one’s argued over the status of Ebola as a disease. But some cases are not so clear. In fact, the criteria for what constitutes a disease, formally discussed as how to classify the pathogenicity of microorganisms, can be found as a lively debate in the medical literature.
So all diagnoses in medicine involve a consensus judgement about what counts as ‘bad for us’. There is no biological test that which can answer this question in all cases. Value judgements are certainly more common in psychiatry than infectious diseases but probably less so than in plastic surgery, but no diagnosis is value-free.
“Psychiatric diagnosis isn’t valid because of the following reasons…”
Debating the validity of diagnoses is a good thing. In fact, it’s essential we do it. Lots of DSM diagnoses, as I’ve argued before, poorly predict outcome, and sometimes barely hang together conceptually. But there is no general criticism that applies to all psychiatric diagnoses. Rather than going through all the diagnoses in detail, look at the following list of DSM-5 diagnoses and ask yourself whether the same commonly made criticisms about ‘psychiatric diagnosis’ could be applied to them all:
Tourette’s syndrome, Insomnia, Erectile Disorder, Schizophrenia, Bipolar, Autism, Dyslexia, Stuttering, Enuerisis, Catatonia, PTSD, Pica, Sleep Apnea, Pyromania, Medication-Induced Acute Dystonia, Intermittent Explosive Disorder
Does psychiatric diagnosis medicalise distress arising from social hardship? Hard to see how this applies to stuttering and Tourette’s syndrome. Is psychiatric diagnosis used to oppress people who behave differently? If this applies to sleep apnea, I must have missed the protests. Does psychiatric diagnosis privilege biomedical explanations? I’m not sure this applies to PTSD.
There are many good critiques on the validity of specific psychiatric diagnoses, it’s impossible to see how they apply to all diagnoses.
How can we criticise psychiatric diagnosis better?
I want to make clear here that I’m not a ‘defender’ of psychiatric diagnosis. On a personal basis, I’m happy for people to use whatever framework they find useful to understand their own experiences. On a scientific basis, some diagnoses seem reasonable but many are a really poor guide to human nature and its challenges. For example, I would agree with other psychosis researchers that the days of schizophrenia being a useful diagnosis are numbered. By the way, this is not a particularly radical position – it has been one of the major pillars of the science of cognitive neuropsychiatry since it was founded.
However, I would like to think I am a defender of actually engaging with what you’re criticising. So here’s how I think we could move the diagnosis debate on.
Firstly, RTFM. Read the fucking manual. I’m sorry, but I’ve got no time for criticisms that can be refuted simply by looking at the thing you’re criticising. Saying there are no biological tests for DSM diagnoses is embarrassing when some are listed in the manual. Saying the DSM is about ‘labelling distress’ when many DSM diagnoses do not will get nothing more than an eye roll from me.
Secondly, we need be explicit about what we’re criticising. If someone is criticising ‘psychiatric diagnosis’ as a whole, they’re almost certainly talking nonsense because it’s a massively diverse field. Our criticisms about medicalisation, poor predictive validity and biomedical privilege may apply very well to schizophrenia, but they make little sense when we’re talking about sleep apnea or stuttering. Diagnosis can really only be coherently criticised on a case by case basis or where you have demonstrated that a particular group of diagnoses share particular characteristics – but you have to establish this first.
As an aside, restricting our criticisms to ‘functional psychiatric diagnosis’ will not suddenly make these arguments coherent. ‘Functional psychiatric diagnoses’ include Tourette’s syndrome, stuttering, dyslexia, erectile disorder, enuerisis, pica and insomnia to name but a few. Throwing them in front of the same critical cross-hairs as borderline personality disorder makes no sense. I did a whole talk on this if you want to check it out.
Thirdly, let’s stop pretending this isn’t about power and inter-professional rivalries. Many people have written very lucidly about how diagnosis is one of the supporting pillars in the power structure of psychiatry. This is true. The whole point of structural analysis is that concept, practice and power are intertwined. We criticise diagnosis, we are attacking the social power of psychiatry. This is not a reason to avoid it, and doesn’t mean this is the primary motivation, but we need to be aware of what we’re doing. Pretending we’re criticising diagnosis but not taking a swing at psychiatry is like calling someone ugly but saying it’s nothing against them personally. We should be working for a better and more equitable approach to mental health – and that includes respectful and conscious awareness of the wider implications of our actions.
Also, let’s not pretend psychology isn’t full of classifications. Just because they’re not published by the APA, doesn’t mean they’re any more valid or have the potential to be any more damaging (or indeed, the potential to be any more liberating). And if you are really against classifying experience and behaviour in any way, I recommend you stop using language, because it relies on exactly this.
Most importantly though, this really isn’t about us as professionals. The people most affected by these debates are ultimately people with mental health problems, often with the least power to make a difference to what’s happening. This needs to change and we need to respect and include a diversity of opinion and lived experience concerning the value of diagnosis. Some people say that having a psychiatric diagnosis is like someone holding their head below water, others say it’s the only thing that keeps their head above water. We need a system that supports everyone.
Finally, I think we’d be better off if we treated diagnoses more like tools, and less like ideologies. They may be more or less helpful in different situations, and at different times, and for different people, and we should strive to ensure a range of options are available to people who need them, both diagnostic and non-diagnostic. Each tested and refined with science, meaning, lived experience, and ethics.

Thanks so much. Exactly that….too many excellent points to recite them all here. Diagnosis is a tool..simply that…oh and I loved RTFM
This is superb, thanks, Vaughan. Am also v much enjoying the linked video from DCP 2017.
But damn. Must not allow “Read the fucking manual” to become my new exasperated expression of first choice. That’s going to be a tough one!
Great thoughts! I started with DSM-II in 1975. I am certain treatment has not kept up with diagnosis. Isn’t that the point? Diagnosis indicates treatment offering improved prognosis. We are not there yet.
Good post. I especially liked this:
“Also, let’s not pretend psychology isn’t full of classifications. Just because they’re not published by the APA, doesn’t mean they’re any more valid or have the potential to be any more damaging (or indeed, the potential to be any more liberating). And if you are really against classifying experience and behaviour in any way, I recommend you stop using language, because it relies on exactly this.”
It is impossible to avoid some kind of diagnosis for mental illness/distress/abnormality, unless we stop talking about it entirely. Even if you were to take the view that all ‘psychiatric’ symptoms were manifestations of distress, you would have created a (very large) diagnosis called “distress”, and you would have some criteria (albeit perhaps unwritten ones) that you’d use to make that diagnosis.
It is absolutely true to say that classification – and the scientific operational definition of behaviours – is central to psychology. It may well be true that classification is central to language. There are, however, two problems with the argument that to dispense with diagnosis means we have to dispense with classification.
First, diagnosis isn’t the same as classification. Although there are a few psychiatric diagnoses that correspond to specific behaviours (‘panic disorder’ is a good example), the vast majority of psychiatric diagnoses rely on the combination or co-occurrence of several phenomena (and qualifying factors). Hallucinations, self-injury, low mood, anxiety, fatigue etc all exist, and are identified, it is in the combination of these phenomena that diagnosis occurs. It is probably in this combination of identified phenomenon that much of the loss of reliability and validity that plagues psychiatric diagnosis also happens.
Secondly, however, diagnosis is a specific form of classification. It is, as the Oxford English Dictionary makes clear, the process of identifying “a disease”. Classification and diagnosis are not synonymous because not all acts of classification include the pathologisation of the subject of that classification.
And, of course, the argument that choosing not to make diagnoses would make it impossible to act scientifically or to use language appropriately doesn’t seem to apply to cosmology – forces and interstellar bodies are not ‘diagnosed’, they are identified, classified and studied, and very successfully, too. Classification may well be central to applied science, diagnosis is a specifically medical matter.
That’s why, in our paper ‘Drop the language of Disorder’ (http://ebmh.bmj.com/content/16/1/2), I, John Read, Richard Bentall and Jo Moncrieff explicitly argued: “There are alternative systems for identifying and describing psychological distress that may be helpful for the purposes of clinical practice, communication, record-keeping, planning and research, such as the operational definition of specific experiences or phenomena. … Surely a description of a person’s real problems would suffice? A description of an individual’s actual problems would provide more information and be of greater communicative value than a diagnostic label.” That is clearly a recognition of the benefits of classification just as much as it is a rejection of diagnosis.
Thanks for this Vaughan, this is a really super summary. There is a lot to criticise about psychiatric diagnosis (I say this as a psychiatrist) but the current debate on its general utility, which as you say seems to have become a professional pissing contest, distracts attention from attempts to actually improve things and adds very little useful.
A number of these points need further debate as they are well made. I wonder if we could do even better by applying test theory and data reduction techniques to develop a dimensional understanding of clinical phenomena; it seems that there isn’t enough exploration of which traits / dimensions / symptoms are discrete (e.g. Anxiety & Depression co-occur; are they the same underlying “distress” phenomenon?), what bad outcomes are they associated with, which as a society we want rid of, e.g. Suicide, lost contribution, diminished relationships, etc.; what comprehensive reliable measures of these phenomena can we develop, merging dimensions that seem to be the same into base Factors; in overall terms, to develop a comprehensive, reliable and valid assessment system based on sound psychometric assessment? Surely this is a project that psychologists could deliver. Structuring assessment might help reliability, as Vaughan says, but such a system would have fully quantified validity, and could be constantly refined, defined against a clear value base -and it would end reification of dodgy concepts through more sound measurement and mathematics. We have the skills.
Many years ago upon entering clinical psychology there was a strong movement to abandon the “medical model” of clinical psychology. As young researchers and clinicians we actually thought this would be the future. There were many strong arguments against an illness-based-model. There still are. However, the movement died a swift death when academicians who mostly fueled the movement finally realized that moving from the “medical” model would make the health insurance industry ecstatic and save them billions. Clinical psychology would lose it’s greatest source of funding. Clients would lose their coverage of therapy if it wasn’t targeted at “illness.” And so the movement rapidly died despite it’s strong benefits.
The problems with the medical model still exist but the insurance model keeps it alive. I and others have never believed it is generally helpful to “see,” label most psychological issues as “illness.” Not helpful for individuals or society. There are ways that psychological interventions, behavioral interventions could be funded, covered without using the medical model, if the motivation and understanding were there. And if the insurance industry wasn’t running the show.
The whole diagnostic model of clinical psychology survives mostly because of the money system and because of the worship of the medical model. And the need for the health insurance industry. The vast majority of psychological, mental, mind/consciousness, behavioral issues could be dealt with without using a medical illness model. Diagnosis of illness would be replaced by more helpful labels and assessments. These tangled issues need to be discussed together. There are many unconscious assumptions and contexts operating in all of this, and they vary across people and cultures.
This is a refreshing critique of the subject, thank you. Constructively, it might have been better to avoid focusing on conditions like stuttering, narcolepsy and sleep apnoea to make some of your general points. Conceptually speaking, these are not exactly mainstream psychiatric diagnoses. Adolescent/adult onset stuttering is explicitly excluded from DSM-5, while childhood onset stuttering is primarily a neurodevelopmental disorder with secondary psychological and social features. Meanwhile, do conditions like sleep apnoea and narcolepsy really belong in a psychiatric diagnostic manual? Their differential diagnoses might include some primarily psychiatric disorders but they are not themselves primary psychiatric disorders.
A more general criticism of DSM-III through DSM-5 is their pervasive innumeracy regarding the diagnostic criteria they present. They never state the discriminating value of any of the criterion symptoms. If those key symptoms were evaluated in the same way that candidate biomarkers have been assessed for sensitivity and specificity then the biomarkers would compare more than favorably. See, for instance, this discussion of Bayesian use of biomarkers in psychiatric diagnosis: http://tinyurl.com/y7h7wtf4. What needs to happen in psychiatry is avoidance of strident but misguided demands for absolutely informative biomarkers, which seldom exist even in general medicine, with a move to incorporating biomarkers along with clinical features, as in the rule in general medicine. And for both the clinical features as well as the biomarkers, let’s get numerate!
Great post Vaughan. I’ve shared it on the clinical psychologist Facebook group, and people very much appreciate your points.
I especially like your RTFM comment, not that I have personally.
Also, people said I should repost the satirical fiction I posted last time we debated diagnoses in the Facebook group, so here it is:
DSM 6 Secret Meeting/Dinner Party/Patriarchy Club:
“I am concerned, gentlemen,” Said Prof Farnsworth, taking a long drag on his Cuban cigar. “The radical left has started to deconstruct our diagnoses, suggesting that people’s difficulties are caused by trauma, distress, and even poverty!”
“That’s preposterous!” roared Prof. Fauntleroy, nearly choking on his Foie Gras, “Everyone knows that the five hundred forms of insanity are caused by chemical imbalance, and the fact that poor people’s brains are abnormally formed! That is why they are poor!”
“Indeed,” interjected Mr Burns, looming into the light from the malevolent shadows, “That is the message we need the proletariat to swallow, if we want to keep selling them mind altering drugs that is.”
“You know who I blame Burny,” added Fauntleroy, in between bites of a roast chicken leg, “Its the Psychologists, and the feminists. THEY are the ones who are poisoning people’s minds against us. We have to DO something about it. I suggest, we create, a NEW DIAGNOSIS!”
Hush descended on the DSM 6 diagnosis working group. The silence was so thick you could cut it with a knife. All the psychiatrists looked to Fauntleroy, hoping beyond hope that his new diagnosis would finally put the Clinical Psychologists in their place.
“I suggest we call it… Irritable Bastard Syndrome, or IBS for short!” he defiantly roared.
“Can’t call it that. Will get confused with Irritable Bowel.” Interjected a bright young colleague, who was a genius but overly pedantic at times.
“Uppity Bastard Syndrome then!” Fauntleroy argued, “Yes,Uppity is even better than Irritable. That way, if one of the psychologists starts talking about childhood trauma, you can just call them Uppity, and suggest a high dose of Risperidone. That ought to shut them up. And if they argue, you can just say they are getting defensive. Use their own terms against them and whatnot.”
The gathering of psychiatrists roared with approval, and within a fortnight, Uppity Bastard Syndrome was in the DSM 6. Soon, clinical psychologists all over the country were diagnosed and medicated. The patriarchy had won…
I found this interesting beyond the specific subject being addressed: in particular– the unique nature of medical diagnosis in general, and the importance of etiology in both physical disease and psychiatric disorders, which differs in many respects from the derivation of ’causes’ in other fields of science.
Thank you. Sense talk a last. I agree with all your points.
Fascinating read. Now I’m wondering why sleep apnea is a psychiatric diagnosis. Is it because sleeplessness causes memory problems? Or because sleep medicine is a branch of neurology…..clearly I missed something.
Sleep apnoea can starve the brain of oxygen and reduces sleep quality, causing cognitive difficulties. It’s one of those definite physical cause diagnoses that has real psychological effects.
The best short term treatment is oxygen at night from a CPAP machine, but the best long term solution is sometimes losing weight, and ironically therapy can help with that. The bio vs psychosocial distinction is often not the best way to think.
Thanks. I guess I’m just confused, other illness like sinusitis, Lyme disease, MS can cause severe or unrelenting fatigue too, so why apnea in particular. I think it’s smart to include these causes, but I didn’t know if they were.
Excellent and very clear. Talking about distress always annoys me. Family member with schizophrenia, currently very out of touch with reality, only thing that distresses her at the moment is insistence that she needs to be in hospital! Friend just been diagnosed with epilepsy on basis of two reported nocturnal seizures. Booked in for CT scan and EEG but results won’t change diagnosis
Vaughan wants us to critique diagnosis more effectively. I agree – and I want us to critique the critiques more effectively as well. With this in mind, I am addressing some of the ‘myths and over generalisations’ in his blog. I’m tempted to say ‘RTFC’ – the final word being ‘critics’ not ‘manual’. Anyone who does this will be aware that:
No one is denying that the heterogenous ragbag of conditions that make up DSM/ICD includes some legitimate medical and developmental disorders, complete with biomarkers, along with a range of other conditions that may be neither ‘mental’ nor physical illness/ disease and which require their own analysis. This really is a tired and desperate argument. If this distinction isn’t always spelled out explicitly in critiques, it is because it is hard to believe that anyone is unaware of it.
In fact DSM and ICD are such a random ragbag that you can demonstrate almost anything by pointing to one or other categories within them. Why are insomnia, erectile dysfunction, stuttering, dyslexia and neurocognitive disorder being cited in this blog? Surely not as examples of ‘mental illness’? But that’s the whole point. Why have we ended up with this bizarre mixture, some of which would be much better filed under disciplines like neurology than appearing in a manual devoted to ‘mental disorders’? When Vaughan says ‘Diagnosis can really only coherently criticised on a case by case basis’, I agree. There is a substantial literature devoted to doing just this – for example, looking at the particular issues that apply to ‘schizophrenia’ as opposed to ‘personality disorder.’
And when we do look at the diagnoses that are (as I am sure Vaughan knows) the actual focus of critiques, his points are largely irrelevant. Thus, he says we can improve the currently ‘atrocious’ reliability figures by using a structured assessment. But where does this get us? Reliability is not validity – we all know this – and the fact that in Biblical times similar populations were reliably identified as being possessed by evil spirits, or in the 17C were reliably identified as being witches, does nothing to validate the categories.
Ditto the argument about categories being decided by committee. The difference – obviously – is that in legitimate branches of medicine, those committee decisions are based on actual medical and scientific findings about bodily functioning, supported by theoretical networks that link signs with symptoms. In contrast, as memorably admitted by a DSM committee member in James Davies’ book ‘Cracked’:
‘What I saw happening on these committees wasn’t scientific – it more resembled a group of friends trying to decide where they want to go for dinner. One person says “I feel like Chinese food” and another person says “No no, I’m really more in the mood for Indian food” and finally after some discussion, they all decide to go have Italian’.
Ditto, also, the argument about ‘distress’ not being a specific criterion in many diagnoses. I have yet to see anyone claiming that it is – but in any case, how is this relevant? The point is that reports of unusual or (often but not always) distressing forms of thinking, feeling and behaviour – even if dressed up in pseudo-medical language – are actually the only way of making these core ‘diagnoses’. This is not a legitimate medical diagnostic procedure. Rather, it relies on failure/refusal to acknowledge the evidence that these reactions are intelligible responses to relational and social contexts.
Ditto the argument that biological tests are used as exclusion criteria in many diagnoses. This in no way proves that the condition you are left with is a ‘mental illness’, nor does it in any way validate the specific label you apply to it. Rather, it tends to prove the critics’ point that ‘mental illnesses’ do not have any biomarkers, and if any are found, the condition instantly turns into a physical illness.
Of course, there are degrees of certainty with which any medical diagnosis can be made, ranging from those based on conclusive biological signs to those which fall on a spectrum and may be based partially on behaviour and self-report. Similarly, the cut-off between ‘health’ and ‘disease’ isn’t always clearcut. But the examples Vaughan gives – spinal tumours, osteoarthritis in the hand, sensory loss, Parkinson’s – are undisputed examples of bodily malfunctioning, and thus rightly regarded as medical illnesses. Citing them is question-begging on a grand scale, since this fact is exactly what remains to be demonstrated in the core psychiatric diagnoses.
I will pick up on a couple more points. Vaughan objects to critics ‘pretending we’re criticising diagnosis but not taking a swing at psychiatry.’ It’s not clear what is meant by ‘psychiatry’ here. To critique diagnosis does have implications for the whole psychiatric system with all its professions, as critics have said. No critics could possibly fail to be ‘aware of the wider implications of our actions’ – that’s exactly what they write about. Individuals take a range of positions on these issues which don’t line up neatly with professional boundaries. But the relevant verb here seems to be conjugated as follows: Vaughan ‘offers a critique.’ Lucy, Peter, Sami and others ‘take a swing at psychiatry.’ Critics ‘treat diagnoses like ideologies.’ I am concerned by a rhetoric which implicitly positions some critiques (Vaughan’s) as necessarily more objective and immune from ideology than others.
And now for the strangest sentence in the whole blog – ‘If you are really against classifying language and experience in this way, I recommend you stop using language, because it relies on exactly this.’ Humans have an infinite range of ways of grouping experiences together, most of which are not formal ‘classification’ in the natural sciences sense. Some of the more helpful ones take the ordinary descriptive form of ‘Hearing voices’ or similar. The problem is not the use of language. It is the inappropriate use of medical language. All human experience has biological aspects. Not all human experience is best understood as a medical illness.
Finally, I will comment on the context in which this blog appeared. There had just been a very bizarre blog – praised by Vaughan – by a non-MH professional, which posed numerous objections to the ‘What happened to you?’ part of the common survivor slogan ‘Instead of asking what’s wrong with you, ask what happened to you.’ In response, it was forcefully pointed out that MH professionals actually have a duty to ask about possible trauma and abuse, and to do so in a respectful and appropriate way as set out in disclosure training. This triggered a dismaying flood of defensive responses from professionals apparently unaware of these responsibilities, along the lines of ‘Not everyone has been abused’; ‘We mustn’t pressurise people’; ‘It will damage the therapeutic relationship’; ‘This is just pushing our own agenda’; ‘We can’t go back to the days when we thought everyone had been abused’ and so on. This is despite recent reviews showing widespread, systematic failure to ask about – let alone address – trauma and abuse in MH services; a collective betrayal that all professionals should be aware and ashamed of. But then along comes Vaughan’s blog! And suddenly the Twitterverse is back on the much safer ground of attacking those misguided ‘critics’ (the most outspoken of whom, ironically, include the very people who drew up these manuals in the first place, and who have described DSM 5 as ‘unsafe and scientifically unsound.’) And while some people lapsed thankfully back into their familiar battle lines, on the very same threads tragic and heartbreaking stories of abuse, unidentified, denied and then compounded by services, obscured and justified by toxic labels such as ‘borderline personality disorder’, were bravely being disclosed… and largely ignored.
Diagnostic labels facilitate denial and re-traumatisation, and are often experienced as traumatising in themselves. We need to face up to this fact. But as we have seen over the last few days, the dynamics of trauma and trauma denial are powerful, and can appear in many different forms.
Hi Lucy,
You’ve written a detailed response, and your views in these debates are always well thought out and quite nuanced. However, this is not always the case with others in some of these debates.
On the RTFC point – I must admit I have not read your published critiques in detail, but I have read your formulation book, and read and thought about your comments, both here and on Facebook. However, I feel that there are also people on the diagnosis critique side that have also not fully considered your arguments, and grossly over-generalise from the points that you make.
For example, I have recently seen people – qualified clinical psychologists no less – arguing that diagnoses are invalid because there is low reliability. They perhaps don’t grasp that validity and reliability are separate concepts, as you so rightly point out here.
I have also seen clinical psychologists questioning the validity of diagnoses, on the basis that they are stigmatising. I quite agree that some diagnoses are stigmatising, but this is a separate issue from validity also. One can be labelled as a murderer – which is very stigmatising – whilst not being an invalid label (unless you are actually innocent).
However, the most frequent statement I see is along the lines of “diagnoses are invalid” or “they are medicalising distress” both of which produce a lot of hits on Google. What this means is that there are people out there who are making such over-general and sweeping comments. On the basis that people who hold such views are unlikely to be persuaded by people who tend to oppose them, do you think you could do more to correct this thinking in people? After all, many of them would say they agree with your views, whilst failing to express the nuances of your arguments.
Of course Vaughan has picked examples with physical causes – just as you and others pick the constructs with the least amount of evidence for physical causes. Lets agree that of the vast amount of diagnoses out there, there is a spectrum of cause from say, traumatic brain injury on the physical end, to certain “personality disorders” at the other. I’m sure we can all agree that there are spectrums of cause, validity, reliability and stigma, which are perhaps overlapping in some places, or separate in others.
Lets also remember that just because someone has a definite physical cause difficulty, that this doesn’t also rule out trauma reactions too. I have a client with an acquired brain injury for whom most of the difficulties can be explained by a psychodynamic formulation of childhood trauma – the ABI is mostly an exacerbating factor rather than the primary cause, even though the client definitely has it.
Finally, I am with Vaughan on the use of language. The problem is that, although the label “depression” is not ideal, and doesn’t capture the fact that everyone’s experience of these kinds of difficulties is unique (as a good formulation does), without such a label we would be in a real bind. How would we Google to find out what other professionals, clients and family members with “depression” do about it if there was no such label as “depression” to put into Google? Without a label such as “Borderline Personality Disorder”, horribly stigmatising though it may be for some people, would Marsha Linehan have been able to develop DBT, which has the most evidence for being effective for this difficulty? How would professionals find out about DBT if there was no BPD label?
As language evolves, stigma evolves too. Do you remember when the Spastic society changed its name to Scope, due to playground abuse of the word?
I still agree with you about potential stigma though. I tend to use psychiatric labels discretely and off the record, as a purely pragmatic shorthand, rather than a conclusion. In doing so I recently found out that a psychiatrist had avoided diagnosing a person with “narcissistic personality disorder” because he didn’t think it would be helpful. He totally agreed with and praised my formulation though, and I learned a great deal from your book on formulation, so your ideas are getting through and helping people.
Dear Lucy,
Firstly, many thanks for your thoughtful comments and taking time to read and respond to my article. It’s much appreciated. Some of my comments below.
The last section about the ‘context’ is a little puzzling I’m afraid. I’m not sure what relevance this has to the points made in my post. However, the piece you refer to was by Dariusz Galasiński, who is an academic linguistic and someone with lived experience of mental health problems. I’m not sure why you dismiss his comments as “by a non-MH professional”. But again, I’m not sure how this is relevant to my specific arguments.
You quote me as saying ‘If you are really against classifying language and experience in this way, I recommend you stop using language, because it relies on exactly this’ and say this is the strangest sentence in the blog.
This sentence is so strange in fact, that I didn’t actually write it. You misquote me. I wrote “And if you are really against classifying experience and behaviour in _any_ way, I recommend you stop using language, because it relies on exactly this.” Obviously, it would make no sense to say ‘if you are against classifying the way the DSM does then stop using language because language relies on classifying experience and behaviour’ which is why I didn’t write it.
You say I’m negatively portraying DSM critics as “taking a swing” but myself as “making critiques”. I literally argue the exact opposite. I say, you can’t separate the two. Everyone, me included, is doing the same.
You write: “the argument about ‘distress’ not being a specific criterion in many diagnoses. I have yet to see anyone claiming that it is”
I quote you in the article saying the DSM and ICD “are about describing people’s distress in terms of medical diagnosis” (taken from your book A Straight Talking Introduction to Psychiatric Diagnosis). In your chapter in Critical Issues in Mental Health you write “Real alternative to psychiatric diagnosis need to avoid the trap of assuming that the scientific categorization of mental distress is possible or necessary at all”. In your chapter titled The Limits of Biomedical Models of Distress for the book Critical Psychiatry you write “Psychiatric theory and practice is based upon a biomedical model – that is, an assumption that mental distress is best understood as a medical illness”. Obviously you’re not alone in this regard, others have made similar arguments.
It therefore seems reasonable to discuss the extent to which the DSM actually does ‘classify distress’. Rather unevenly it seems.
You say that committees from “legitimate branches of medicine” makes decisions based on “actual medical and scientific findings about bodily functioning, supported by theoretical networks that link signs with symptoms” and cite James Davies’ book ‘Cracked’ to say the DSM committee resembled a group of friends trying to decide where they want to go for dinner.
It’s hard to know how to respond to this. The papers of the diagnostic working groups across medicine are published in the medical literature. You can read and compare them. You may be surprised to learn that restaurants feature remarkably infrequently in any of these discussions. It could of course be that the DSM committees publish these papers full of evidence and scientific findings but then get together, ignore them, and just exchange personal preferences but it’s highly unlikely. If this did happen with the DSM, it’s curious to think how many biomedical tests actually made it into the manual. Maybe someone left their blood test results in the takeaway menu?
But as I mention, diagnoses as decided by all diagnostic committees are not solely based on evidence from medical tests. All involve value judgements, opinion and debate – not only about the body but about the wider effects of changing diagnoses on practice, society and public opinion. Again, this is all public record.
You ask “Why are insomnia, erectile dysfunction, stuttering, dyslexia and neurocognitive disorder being cited in this blog? Surely not as examples of ‘mental illness’?”
I don’t mention mental illness once in the blog. I’m addressing bad arguments against diagnosis. One of the source of bad arguments is having an implied list of ‘what count as psychiatric diagnoses that I consider legitimate targets of my criticisms’ without it ever being declared.
I mention neurocognitive disorder solely when noting the relation between biological tests and DSM diagnoses of various sorts. I don’t claim it’s a mental illness or functional diagnosis at any stage.
The diagnosis of insomnia (Insomnia Disorder in the DSM-5) is based on self-reported symptoms, including self-reported dissatisfaction and sleep quality. It is not based on what you call “medical and scientific findings about bodily functioning”. It’s hard to say why you would consider depression, for example, to be an invalid diagnosis but insomnia to be a valid one when the same criticisms you make against depression also apply to insomnia.
Erectile disorder is where you can’t get an erection in the absence of individually identifiable physiological problems. Stuttering is where you have problems with speech fluency in the absence of any identifiable physiological problems. Dyslexia is where you have problems with reading in the absence of any identifiable physiological problems. They are purely diagnosed on self-report and behaviour.
You say identifiable physiological problems are necessary for something to be a legitimate medical diagnosis but these DSM diagnoses don’t fulfil that criteria and yet you consider them legitimate.
This could either because your argument is flawed, or it could be that you have a certain set of diagnoses for which your argument applies. I’m really happy if it’s the latter. In which case, just say, “here are the diagnoses for which my following arguments apply”. Basing criticisms of diagnosis on ‘we all know what we’re talking about don’t we’ just means we don’t know what you’re talking about, and your arguments, rightly or wrongly, seem incoherent.
So nowhere do I address the definition of ‘mental illness’, I’m just asking for clarity on arguments about diagnosis.
You call the DSM and ICD a “heterogenous ragbag of conditions”. The DSM maybe (in fact, I have argued this myself) but it makes no sense to call the ICD the same. It aims to be a comprehensive list of all medical diagnoses. Clearly, I wouldn’t point to different categories in the ICD to make comparisons about psychiatric diagnoses because it isn’t limited to psychiatric diagnosis. That would make no sense. The DSM is a psychiatric diagnostic handbook, however, so if someone criticises psychiatric diagnosis as a whole, it makes sense to look for inconsistencies in the presented arguments based on what are actually formally and explicitly defined as psychiatric diagnoses.
You are right that reliability does not imply validity but the latter depends on the former. You can’t have a valid diagnosis that is also unreliable. So where does it get us? It helps establish one of the necessary but not sufficient conditions for validity. You have stated many times that psychiatric diagnosis cannot be made reliably. This is not true as I show. This doesn’t mean automatic validity, but hopefully this addresses one of your specific claims.
You say “the examples Vaughan gives – spinal tumours, osteoarthritis in the hand, sensory loss, Parkinson’s – are undisputed examples of bodily malfunctioning, and thus rightly regarded as medical illnesses. Citing them is question-begging on a grand scale, since this fact is exactly what remains to be demonstrated in the core psychiatric diagnoses.”
Again, ‘core psychiatric diagnoses’, I don’t know which you consider core.
However, I cite these specifically when addressing the argument that psychiatric diagnoses are illegitimate because they’re unreliable, or, are based on experience and behaviour, and show how diagnoses of other undisputed medical conditions are the same. So no question begging.
You write “The point is that reports of unusual or (often but not always) distressing forms of thinking, feeling and behaviour – even if dressed up in pseudo-medical language – are actually the only way of making these core ‘diagnoses’. This is not a legitimate medical diagnostic procedure.”
As I note in the article, this applies to many non-psychiatric diagnoses: tinnitus, sensory loss, many pain syndromes, headache, vertigo and the primary dystonias but there are many more.
Presumably, you think these should also be abandoned as illegitimate because they’re not based on legitimate medical diagnostic procedure? From your arguments it seems so, if not, some clarity would be good.
In conclusion, I think what you do Lucy is extremely valuable. We need ethically minded motivated critics of diagnosis. I’m just keen that we’re refining our arguments and being clear about what we’re discussing. Without this, progress is limited and conflicts arise based on ideology more than the substantive issues.
I’m not out to ‘defend psychiatric diagnosis’ – in reality, I think lots of them are a bit crap. I’m actually a diagnosis agnostic, and I want to see whether each is useful on a case by case basis.
I’m am, however, a believer in having useful tools available to people who want help and a believer in the use of debate as a way of doing this better. So thank you for participating here – it’s always greatly appreciated.
Yours in partnership for better mental health,
Vaughan
Supposedly these don’t label distress…
“Here is a non-exhaustive list: Schizophrenia, Tic Disorders, Delusional Disorder, Developmental Coordination Disorder, Brief Psychotic Disorder, Schizophreniform Disorder, Manic Episode, Hypomanic Episode, Schizoid Personality Disorder, Antisocial Personality Disorder, and so on. There are many more.”
I think the writer has a deficient understanding of distress if they don’t see this list as consequences of distressing experiences.
t is very revealing how much resistance there is to discuss the issue of “money” when discussions of diagnosis occur. It is a hidden issue in the room that people don’t want to see. Likewise, it is revealing how much reluctance there is to discuss the human mind/brain issues with perceiving something as an illness or not an illness. Why isn’t there more discussion and curiosity about what the brain/mind, what the internal machinery of humans is doing underneath. Human brains/minds have the ability to hugely influence the “objects” being perceived. But the focus is almost always on what are those human’s beliefs, feelings, attitudes, behaviors, understandings, reactions, etc., etc., to the object, without any analysis or discussion about how the “objects” being reacted to are hugely different between various humans. People are reacting to different statues….and nobody points that out or discusses that that is something our machinery does. It is what human machinery does.
Don’t just ask me what are my beliefs, opinions, reactions, feelings, actions, desires…etc…. Also Ask me what my brain/mind has created as the “object” I am reacting to. We’re ignoring our own machinery and only looking at it’s outputs. We can teach ourselves and others to study reactions but also include study and curiosity of what our brain/mind created as the objects of perception. (what is the statue my brain/mind created that I am reacting to….What statue did your brain/mind create that you are reacting to????)
This is relevant to this discussion, any discussion when there seems to be puzzling disagreement. Include talking about our “machinery” that influences what is (are) the object(s) that have our reactions and positions? What is the underlying machinery operating underneath the beliefs, values, understandings, feeling, actions….etc? We can be taught to do this. We can teach average people to include this in their process. Not just what are my beliefs, opinions, feelings, reactions… etc… etc…. but also what has my mind/brain done as part of this. We can bring that later issue into conscious awareness and discussion, instead of it just operating in the background, out of consciousness and out of discussion.
What statue am I reacting to? What statue are you reacting to? Alien Anthropologists would be puzzled about humans not taking their own human nature into account when living their lives and struggling to understand themselves and others.
This is relevant for both those being diagnosed and those doing diagnoses. Or we can pretend the statues are the same.
Yes, we do need to get better at critiquing psychiatric diagnosis. Yes, there are unhelpful generalisations made in the wide, complex and evolving body of work and activism which critiques diagnosis. Yes, there is much thoughtful debate still to be had by those of us who see and experience problems with the diagnostic approach to emotional difficulty. Resorting to rhetoric and obfuscation is not a helpful way of improving that debate.
Indeed, so much in the blog swirls so loosely and disconnectedly around the central arguments it professes to address, that a detailed response would run the risk of failing to engage with the central points. Lucy Johnstone’s excellent response above points out that the DSM/ ICD constitute a “heterogenous ragbag of conditions” – a point of critique in itself. Vaughan is clearly a well-informed writer and will surely be aware that the critique of psychiatric diagnosis centres on conditions such as schizophrenia, anxiety, depression and personality disorder – those other conditions which form the vast bulk of psychiatric practice and experience. To call on biochemical markers for obstructive sleep apnea hypopnea, or to posit rhetorical questions about the usefulness of the diagnosis of pica, seems a rather wilful confusion of the issue.
Vaughan will also be well aware that the argument that there is no biological cause of, or biochemical marker, for anxiety, depression, schizophrenia, PD etc is a central plank of many critiques of psychiatric diagnosis. I’m sure that I would be underestimating his intelligence to infer that he isn’t aware that there is a distinction between biochemical markers of a condition; and carrying out biological tests in order to prove that other conditions aren’t present. Yet the blog indicates otherwise. So far, so confusing.
With Vaughan’s evident intelligence in mind, I cannot bring myself to believe that he is not aware that the simplified, generalised argument that diagnosis “medicalises distress” is not based on the misconception that every psychiatric diagnosis has “distress” as a criterion. Rather, it refers to the way in which diagnosis identifies the individual’s pathology as the issue – rather than the ways in which that individual has been shaped, socialised, traumatised, damaged or otherwise affected by experience. Even more confusing. Perhaps Vaughan needs to RTFC – read the fucking critique – with a little more depth and attention?
Perhaps this confusion is in part explained by the fact that, in this morass of fact and statistic, the blog simply overlooks the experience behind the critique of diagnosis – not least the experience of the average psychiatrist who, I am fairly sure, does not have a case load consisting primarily of people seeking treatment for their diagnoses of pica, erectile dysfunction and sleep apnoea.
I have a diagnosis of Borderline Personality Disorder. I am also a “homosexual”. Before 1968, my homosexuality could have been diagnosed – arguably with reliability and validity. It does not mean that it is, or ever was, morally or politically justifiable to frame my sexuality as an illness. Nor can anyone can argue anymore that such a diagnosis was a positive experience for the individual – or for society. An obvious point, perhaps, but one which is present in many critiques of psychiatric diagnosis, and bewilderingly absent from this blog.
Vaughan points out, rightly, the diagnosis of physical illness and disease is often partial, complex and subjective. He makes the point that “all diagnoses in medicine involve a consensus judgement about what counts as ‘bad for us’. There is no biological test that which can answer this question in all cases. Value judgements are certainly more common in psychiatry than infectious diseases but probably less so than in plastic surgery, but no diagnosis is value-free”. Right so. The critique of psychiatric diagnosis has not been developed for the sake of argument or point-scoring. It is – often overtly – based on values, and has been informed by the damage wreaked by diagnosis: which in part, has been the positioning of individual pathology – chemical imbalance and faulty genes – as that which is “bad for us”, rather than the experiences which lead to suffering and difficulty (please excuse my simplified and generalised language).
I’m not at all interested in inter-professional rivalries. I’m motivated by the belief that helping people in distress and difficulty should involve listening to and caring the individual; seeing and responding to them as a whole person; taking into account all past and current aspects of their lives which have contributed to their current difficulties; and at the very least, seeking to avoid doing further harm. And so to language.
I am glad that Vaughan recognises the complexity of language, which does not just express but also construct our experience of the world. Quite right. How do I understand or communicate my experience of the table without naming it as “table”? The question of how we find commonalities with other people who share our experiences without using labels is a complex debate. However, it is quite another thing to draw on a kind of postmodern relativism to sidestep responsibility for how and why we label people; and the impact that those labels have. It is one thing for me to name that I am feeling depressed; and another thing for me to have “depression”. It is one thing for me to find commonality with other survivors of sexual abuse who self-injure in order to cope with difficult feelings; and another thing for me to be diagnosed with Borderline Personality Disorder; a diagnosis which – at its linguistic core – is inherently damaging. All language has consequences. I am optimistic enough to believe that professionals and theorists have the intelligence and empathy to use language with care; and to recognise when linguistic frameworks are too problematic to be put to good use.
I’ll close here, because all of the points I’m making have already been made and continued to be made with much more power – and infinitely more complexity – by others in the psychiatric survivors movement, Mad Pride, Hearing Voices, Rape Crisis, the many and varied voices of second and third wave feminism, the debates in the self injury movement, the various movements compromised by survivors of trauma and abuse, the multiple thoughtful activists and authors of the peer support movement, the fascinating and evolving cross currents of the disability rights movement, civil rights movements, BAME movements, LGBTQ people …..
You get my point. RTFC, Vaughan.
Dear Clare,
Thank you for engaging with my article in such depth. I’m not going to respond in excessive detail because I’ve addressed some of the points you make in reply to Lucy above. However, you make a really good point when you say (to paraphrase) that I’ve not addressed some of the most substantive criticisms against diagnosis.
This is true. There are many good criticisms of certain psychiatric diagnoses. I have made many myself over the years, and I would like to think some of them will stand the test of time.
However, I didn’t set out to defend diagnosis, nor specific diagnoses. The blog was directly addressing bad arguments against diagnosis. So no, I didn’t address or attempt to refute some of the better arguments against certain diagnosis (for example, the risk of de-contextualising and de-legitimating lived experience – which you describe so lucidly) largely because I agree with them.
I would disagree with one specific point you make though. You suggest I’m not “aware that there is a distinction between biochemical markers of a condition; and carrying out biological tests in order to prove that other conditions aren’t present. Yet the blog indicates otherwise.”
I don’t think it does. I simply discuss all the ways in which biomedical tests relate to DSM psychiatric diagnoses – from no relation at all to being entirely based on biomedical test results and everything in between, including, of course, exclusionary test results. Clearly I am aware of this distinction, which is why I make it explicitly in the article.
Perhaps to a more central issue though, I think the arguments you make about the potential for diagnoses to do damage are entirely valid. The voices of people who have been harmed by diagnoses are, sadly, greatly under-valued and too often side-lined. I hope we can move towards discussion and inclusive debate to better highlight this and move us forward.
Many thanks for your insightful comments here, they’re much appreciated.
Yours in partnership,
Vaughan
I see Lucy persists with her false dichotomy between medical and psychiatric dx After spending 3-4 years examining the evidence there is overlap between these dx in terms of validity, reliability, clinical utility etc Many medical dx are based on judgments Some do not rely on objective evidence of disease Some are based on experts deciding thresholds.
Of course we do not have objective measurements of eg thoughts or emotions hence the lack of diagnostic tests for “functional” MH dx
As for illness it is a messy term that is different but overlaps with disease another messy term
Medical practitioners also can be helpful in conditions that are not diseases or illness.
The tendency of critical MH to say psychiatry is not a part of medicine is the same reason the British declared the Bengalis a non-martial race – a false statement made for reasons of gaining power
Brilliant piece of writing, Vaughan. Thank you for this important treatise.
It is refreshing to see the opacity of the generic term ‘distress’ cleared away, and the rationale for a practical (if flawed, like all classification systems) system of shared language elucidated so well. You debunk much of the mythology about diagnosis, and focus on not just the utilitarian aspects but also the vital importance of diagnosis to the many people for whom it has helped, often in a life changing, progressive, way.
As a neuropsychologist, I often hear from critical psychologists that people with neurological disorders are ‘different’ and therefore have no voice in this debate. This is an attitude which, historically, has excluded people with brain injury, stroke, Parkinson’s, MS, Epilepsy, and even FND, from access to mental health services. To see that psychologists maintain this view in 2017 is disheartening, to say the least, and I believe your article is a significant contribution to dissolving the barriers that evidently still exist.
Trauma of a different kind. Child knocked down by car, sustains complex skeletal and soft tissue injuries. Contexts: world in which cars dominate over pedestrians; behaviour of drivers; design of cars and roads, crossings etc.; supervision/care of child; play facilities for children; response of emergency services; that child’s prior development. But still need to understand a) precise nature of injuries involved, and underlying anatomy and physiology, in order to treat in best way b) the nature of the psychological impact (including that of hospitalisation), which will depend on many other factors, in order to help in the best way. It is not diagnosis vs understanding of trauma, it is BOTH
Following our brief Twitter exchange, I thought it best to leave a much more detailed comment here.
Overall I found your blog disingenuous, misleading and – intentionally or otherwise – a defence of the status quo in regards to biomedical dominance within mental health services.
But first my points of agreement with your article. I welcome you highlighting the unreliability and guesswork associated with some mainstream medical diagnoses, where committees decide – often under pressure from the pharmaceutical industry – to change (typically expand) the range of biological measures assumed to be indicative of pathology. Examples of such a process pertain to deciding on values indicative of high blood pressure and cholesterol levels. You also make the valid point that power is very important in the mental health sphere and that the DSM contributes to maintaining psychiatry’s privileged position within it. (Although the common cry of ‘turf wars’ from some vocal supporters of the biomedical approach is an inaccurate distraction, an avoidance of discussing the pertinent issues; as this blog – and the subsequent comments – show, some strong advocates for biological psychiatry come from the clinical psychology profession).
The reasons for my ‘disingenuous’ and ‘misleading’ conclusion include the following:
1. Given the title of your blog, it is reasonable to assume that you were addressing the mainstream psychiatric problems of ‘schizophrenia’, ‘depression’, ‘bipolar disorder’, ‘personality disorders’ etc. Of course, common criticisms of psychiatric diagnosis do not apply to all the ‘disorders’ in the hotchpotch that is the DSM. Given your clinical and academic experience, I’m sure you are fully aware that controversies do not concern such things as erectile dysfunction, stuttering, sleep apnoea and narcolepsy.
2. Whether or not ‘distress’ is, or is not, a stated criteria of a ‘disorder’ within the DSM hardly seems relevant here. When critics talk about ‘medicalising distress’ the broad meaning is clear: the unhelpful reduction of human suffering and overwhelm to an illness category comparable to those recognised in the physical health domain.
3. Your arguments about higher levels of reliability if structured interviews are used seems, again, of little relevance to the central debate. In practice, such protocols are rarely deployed outside of formal research studies and, as you know, even if higher reliability could routinely be achieved in clinical practice, it would not make the concept of a diagnostic label any more useful – we could all reliably agree what Santa Claus might look like, but this wouldn’t enhance the validity of the notion.
4. Off course all language classifies to some degree, but are you seriously suggesting that there are no differences in the consequences of using everyday descriptive language (e.g. ‘she is hearing voices that distress her’) and diagnostic language (e.g. ‘she’s got schizophrenia’)?
5. Stating that medical tests are sometimes used to exclude psychiatric diagnoses seems of questionable relevance to the debate; it doesn’t mean that what is left constitutes a bona fide illness. And if any of these medical tests do come back positive, the problem becomes something outside of psychiatry’s remit – thus, referring to your example, if someone suffering panic attacks is found to display hyperparathyroidism s/he would immediately become the concern of the endocrinology speciality.
6. Those critical of the biomedical approach recognise that some people value a diagnosis and, of course, we should respect this. Like you say, ‘we need a system that supports everyone’. But this is not what the ongoing –often heated – debate is about. Rather it’s in regard to professional services, media, charities and others with power/influence promoting a biomedical framework as if it’s the way it is, a factual reality, where ‘depression’ becomes comparable to diabetes with an assumed, primary biological cause.
As illustrated above, I mostly view your efforts to debunk criticisms of psychiatric diagnosis as straw man arguments. However, even if your criticisms were legitimate, I still think you are focusing on peripheral issues and missing the key points. As an extrapolation from physical health, DSM diagnoses, however they’re defined, promote ‘illness like any other’ approaches along with all the disadvantages for service users that go along with them: more stigma; less hope; greater passivity; a disregard of adverse life experience; and a gross overuse of psychotropic drugs (leading to often damaging, sometimes catastrophic, consequences). Furthermore, the language of ‘disorder’ used throughout the DSM encourages the ‘illness like any other’ mantra, and dubious assumptions about underlying biological pathology, which in turn exacerbate these disadvantages. When you add to the mix the well-established conclusions that diagnoses are weak predictors of the course of a problem and do little to guide effective interventions, one is left to question whose interests are being served by retaining DSM – it, undoubtedly, is not those of service users.
Which, finally, leads me to question the primary motivation for writing this article. Why strive to highlight and refute invalid criticisms of the currently dominant (and hugely damaging) paradigm, one that fundamentally discriminates against people with an assumed ‘mental disorder’? It seems a bit like trying to find baseless criticisms of apartheid in 20th-century South Africa.
Dear Gary,
Thank you for your comments. To address some of your points:
1. This relies on the “we all know what we’re talking about, don’t we?” approach and I show how this leads to contradictions and logical inconsistencies.
2. This also relies on the “we all know what we’re talking about, don’t we?” approach.
3. My point was that psychiatric diagnosis can be reliable, contrary to prior claims that they can’t. I work and have worked in several clinics where structured assessments are the norm. I’m not here to defend bad practice.
4. I’m not seriously suggesting it, no.
5. At no point do I argue that exclusionary tests therefore prove a bona fide illness. In fact, I don’t talk about whether diagnoses represent bona fide illnesses at all.
6. The debate is about lots of things. I’m only addressing the bad parts of it. I’m not attempting to defend diagnosis, I’m addressing bad arguments against diagnosis.
However, as you suggest this is like me defending apartheid in 20th-century South Africa, forgive me if I keep my response a little brief!
Yours in partnership,
Vaughan
To analyse this argument, we need to be clear on the proposition that the author is advocating. The blog is explicitly arguing that “we need to get better at critiquing psychiatric diagnosis”. There are two ways of understanding this statement which, I believe, has caused some confusion in the debate following the publication of Vaughan’s blog. Firstly, it could be understood as a circumspect proposition that there are some bad arguments against psychiatric diagnosis. There is evidence of this interpretation from Vaughan’s defence of his blog on Twitter when he says that he is “just tackling some bad arguments” and “only addressing bad arguments”. Therefore, we are justified in attributing to Vaughan a narrow proposition that some critical mental health arguments need sharpening.
If Vaughan is restricting himself to this meaning of the proposition then it represents a rather limited challenge to those who criticise diagnosis. It’s a truism to say that there are bad arguments for and against almost any proposition. To illustrate this point, we could to take an example from politics that echoes more polemic positions on diagnosis. We could justifiably claim that, “there are some bad arguments against totalitarianism”. Of course, I could look in the literature and find some bad arguments, and critique them in detail. However, without attending to stronger arguments (for example, those of Hannah Arendt, Isaiah Berlin or Michel Foucault) I am not constructing a robust challenge against those who defend totalitarian thought. The much more challenging proposition, is that arguments against totalitarianism, which are commonly assented to be strong, are flawed.
When Vaughan says that “we need to get better at critiquing psychiatric diagnosis”, I suggest that he is trying to make a stronger point. This more challenging proposition would be that the approach to criticising diagnosis needs to be improved. There is evidence that Vaughan wants to draw wider conclusions when he says that “we should be working for a better and more equitable approach to mental health”, asks “how we can critique diagnosis more effectively”, and claims that “we’d be better off if we treated diagnoses more like tools, and less like ideologies.” However, in order for an audience to be persuaded of a stronger proposition, they need to be presented with arguments that the strongest positions also fall short. In addition, refuting the strongest arguments against diagnosis is also essential for people like myself who may not be aware of the broad literature on mental health. As a trainee psychologist, I want to learn from more experienced service users, academics and clinicians. I expect the debates to represent and select the strongest arguments both for and against a position so that I can make up my own mind. This form of argumentative virtue is essential for moving our debates in mental health forward.
In conclusion, then, either Vaughan is making a very well argued but rather limited assertion that some people make poor arguments against diagnosis, or a less well defended but more challenging argument that there is something limited about the general approach to arguing against diagnosis. I think that he wants us to accept the latter but only gives reasons for believing the former.
Superb. I’d like to translate your post to Russian and repost it in one or two local neuroscience/psychology blogs. Are you OK with that?
Of course. Thanks for asking but no permission needed. Everything we write here is published under a Creative Commons license: http://creativecommons.org/licenses/by-nc-sa/3.0/
As long as health insurance and treatments have to be directed at “illness” we will continue to have diagnosis of illness instead of assessment of problems and assessments of people that help them deal with problems. Follow the money….. treatment money….. and secondarily the money associated with the pills. Unless your anxiety is considered an illness or disorder in DSM you won’t get treatments or at least financial coverage.
Thank you, Vaughan, for your interesting blog which seems intended to help those of us who criticise psychiatric diagnoses, amongst whom you seem to include yourself, to make sure our arguments are in good order. I would certainly concur with some of your comments about the misguided arguments of some criticisms – e.g. regarding the issue of committee judgments about diagnoses in various branches of medicine. Despite this however, I don’t believe your responses to the various lines of criticism successfully rebut the main thrust of the case against psychiatric diagnoses.
In particular, I’m very puzzled by what I take to be the main strategy underlying your arguments. Right at the start of your blog, you state explicitly that you have been a long-term critic of psychiatric diagnoses and you appear to endorse this later on, though with some qualifications. Having stated this position, you then seem to pursue a strategy which tends to cast doubt on whether you really mean it. The central thrust of the arguments against psychiatric diagnoses is that, in most cases, they are unlike medical diagnoses in important ways. You, however, seem to want to demolish this type of argument as far as possible. You may be right to do so, but I think you own arguments here are questionable.
Firstly, in order to pursue your argument you rely on an astonishingly broad conception of what sorts of things are covered by the term ‘diagnosis’. You list things (e.g. in your reply to Lucy Johnstone, and elsewhere I think) such as tinnitus, vertigo, stuttering, and headaches as diagnoses. HEADACHES, for God’s sake??!! Is that really a ‘diagnosis’?? If it is, then we would seem to have lost all hope of distinguishing between symptoms and diagnoses….
Your other examples here are equally dubious. If you’re right about this, then I’ve just discovered that I’ve got one or two diagnoses I never previously knew I had! I actually have tinnitus – I’ve had it for nearly 40 years, but never before thought of it as a ‘diagnosis’. When I went to the ENT specialist and explained the buzzing in my ears, I was just told “That’s called ‘tinnitus'” – i.e. a shorthand name for the symptom. A real diagnosis, which was never forthcoming (obviously there are limits to what medical science can reveal), would have given me some kind of explanation, if only an incomplete one, for the symptom. Also, by your argument, I have discovered I have a ‘diagnosis’ of ‘stuttering’, or at least I used to (much improved now). Again this is a symptom, not an explanation, even if it might be listed as a diagnosis in DSM-5 (I don’t know – I haven’t read the f***ing manual on this!).
At this point, I’m hearing voices (imaginary ones – I’m not hallucinating) telling me that diagnoses in medicine are not necessarily explanatory to any degree at all. That strikes me as a strange view and one that can be questioned in general terms, even if there are a few exceptions. In any case, that requires a lot more argument, which I can’t pursue here. However the point is that this is a central argument in the case being made against the validity of psychiatric diagnoses, and one which you evidently want to undermine, despite your stated stance of being a critic of such diagnoses.
Secondly, and following from this, you argue that there is no significant distinction to be made between medical and psychiatric diagnoses. Obviously if we accept your conception of ‘diagnosis’, then we seem pretty much committed to accepting your conclusion; but as I’ve just argued above that conception is highly questionable. What you also seem to do to support your argument is to downplay the relevance of biomedical tests and results in forming medical diagnoses. It has already been pointed out by others here that you’ve failed to show that biomedical tests are a necessary part of psychiatric diagnoses – all you’ve shown is that they’re often used to exclude other known medical diseases which would then fall under the relevant medical specialty. You seem to suggest, unless I’ve misunderstood you, that the fact there is often (perhaps always) some indeterminacy in the specific measure of the biomedical variable concerned in making the diagnosis entails that such biomedical markers are not essential to the diagnosis. You talk about illnesses not being “cut and dried”. However this is irrelevant. It doesn’t need to be specified precisely how much cardiac troponin is present in the blood stream before myocardial infarction can be diagnosed – just that the level of troponin is raised. Similar considerations apply to the use of imaging results in the diagnosis of lung cancer. So I think a clear case can be made that biomedical markers or abnormalities are an important part of diagnosis in acute medicine in a way that cannot be said of psychiatric diagnoses. Even when such tests aren’t available, there is often evidence of biomedical abnormalities which are known to be a factor in causing the disease.
Thus for example, regarding Parkinson’s disease, you say “..there are no biomedical tests that confirm the condition, despite the fact that studies have shown it occurs due to a breakdown of dopamine neurons in the nigrostriatal pathway of the brain”. On the face of it, this seems a contradictory statement, since you say clearly that biomedical abnormalities are implicated in the disease. Maybe you just mean that no tests can yet identify it, but the biomedical basis is there nevertheless. You also accuse critics of just focussing on infectious diseases in their view of medical diagnosis. However, similar arguments can be made about all sorts of diseases, including autoimmune diseases, cardio-vascular diseases, etc.
In conclusion, I agree with your view that psychiatric diagnoses should be subject to critique on a case-by-case basis, due to the massively varied range of conception of such diagnoses. An all-encompassing critique is bound to meet objections. Nevertheless, I can’t help wondering whether you really mean it when you say you are a long-standing critic of these diagnoses. Your arguments seem more consistent with an approach based on an acceptance of the overall diagnostic framework, with criticisms of individual diagnoses being based on a much more gradual and iterative basis within the conventional disease-model paradigm.
Hi Richard,
I think there is a fundamental misunderstanding about what diagnosis means, amongst those of us that are not medical professionals, i.e. medical doctors.
Many of us would seem to think that a diagnosis of an illness means that we know what the *cause* of that illness is. We also seem to think that the word *illness* or *disease* implies that it is in some way biological in terms of cause. On this basis, we tend to criticise the whole concept of psychiatric diagnoses, either en masse, which Vaughan rightly objects to, or on a case by case basis, which is far more sensible, on the basis that, for example, we don’t know the exact biological causes for certain diagnoses.
This would be a valid argument if diagnosis meant that a thing was an “illness” or “disease” which was *biological* and that it was biologically *caused*. However, this is NOT what diagnosis means. Diagnosis means a cluster of symptoms, which occur together, which we give a name, so that different doctors and other medical professionals can agree on what we are talking about. Diagnosis is just supposed to be a name for a thing. It enables that thing to be studied, searched for on Google etc… It does not automatically mean that the cause is known, or that the cause(s) of that thing are biological.
Of course, for a lot of medical diagnoses, we do know what the cause is, and that cause does tend to be biological. Vaughan makes the point about Parkinson’s being caused by a breakdown of dopaminergic neurons. He’s right about this. However, this STILL doesn’t mean there is a biological test that can diagnose (i.e. name) the condition, because you can’t chop someone’s brain open while they are still alive to look at their dopaminergic neurons in the striatum. Its the same with some forms of dementia which are not obvious from a CT or MRI head scan, but can be noticed (and diagnosed) after autopsy.
Lets take a really contentious psychiatric diagnosis, like “schizophrenia”, as an example. Because there are so many symptoms involved, people rightly question the validity and reliability of the diagnosis, because one person experiencing “schizophrenia” can experience very different symptoms from another. So validity and reliability of *this particular diagnosis* are sensible and vital to people who have this diagnosis.
There is a big argument about cause here also. There is lots of research into the effect of certain genes, but the contributions seem small. “Schizophrenia” is not a simple condition like Huntingtons, caused by a single faulty gene. Conversely, there is lots of research into trauma having been experienced by people with this label. This is important too. There is also research into drug induced psychoses, which are often misdiagnosed as “schizophrenia”, as well as some that argue that drugs such as cannabis can cause “schizophrenia”. The argument about cause is actually separate to the meaning of diagnosis however – all diagnosis means is that those diagnosing agree that the cluster of symptoms resembles the thing called “schizophrenia”. Sometimes they disagree (poor inter-rater reliability) but this is not about cause, or biology, only whether we agree on naming a thing.
Now here is the interesting part. Since 2007, we have discovered a condition called NMDA receptor auto-immune encephalitis. In its early stages, it is a form of psychosis, with hallucinations and extremely disturbed behaviour. In this condition, the immune system attacks certain receptors in the brain, causing swelling, and a whole bunch of symptoms. I met a person who had been very acutely unwell with this illness for the first time in my career recently. Initially, the person had been diagnosed with a psychotic illness, and put on antipsychotic medication, designed to managed conditions like “schizophrenia”. Fortunately, the psychiatrists caring for this person then noticed another symptom, seizures, which are not part of the cluster of symptoms which define “schizophrenia”. They then realised that *something else* was happening, and referred to a neurologist, who ordered a blood test, which confirmed the presence of the NMDA antibody, confirming a diagnosis of auto-immune encephalitis. Auto-immune encephalitis is both a name for a cluster of symptoms (i.e. a diagnosis) but also a diagnosis for which we know there is a cause, and for which we know the cause is biological in origin. I’m pleased to say that after a course of steroids, and some neuro-rehabilitation with myself and my team, this person made a good recovery.
The point is that, prior to 2007, all cases of NMDA receptor auto-immune encephalitis did not yet exist, and were all named “schizophrenia”, a condition for which we do not know the precise causal nature, biological or otherwise, although there are lots of theories and arguments out there (and rightly so). The second point is that, post 2007, we now know that about 1% of what we used to call “schizophrenia” is in fact this new condition. So, as well as the new condition being a precisely defined, medically caused illness, the label of “schizophrenia” becomes slightly less vague, better defined, and more reliable (although only by 1% or so). The third point is that, prior to 2007, about 1% of “schizophrenia” really did have a purely biological cause, its just that we didn’t know what it was yet. The fourth point is hypothetical – we might discover more biological causes for “schizophrenia” in the future, which account for another few percent of cases, and slowly salami slice the diagnosis of “schizophrenia” into more precise diagnoses.
So far, this agrees with the validity and reliability arguments about diagnosis as they relate to “schizophrenia”. Its right to critique the notion that it is all biologically caused, but as the example above demonstrates, some of it was biologically caused all along. The problem is that, as these new narrow diagnoses chop away a little bit of what used to be “schizophrenia” the cases that still attract the label are still unknown in terms of cause, and still lack great validity and reliability, because we don’t know the exact cause.
But here is the problem for people that wish to do away with psychiatric diagnostic labels. What are we going to call the thing in the meantime? I agree with my clinical psychologist colleagues who say that we should always seek to formulate an individual’s difficulties. I do so myself. But in the meantime, we need a convenient short-hand label for things, even things as controversial as “schizophrenia” while we figure out what the hell it is, what causes it, and if it is in fact several different conditions that have different causes, biological or otherwise.
The exact same argument can be applied to more labels like “depression” or “anxiety”.
Remember too that people who heard voices in medieval times were assume to be suffering from “possession” this was also a label, albeit an even less valid one. For all its faults, “schizophrenia” represents scientific progress in understanding reality.
Notice that these arguments are entirely different from arguments about whether specific psychiatric diagnoses are stigmatising or not. That is an entirely different argument, and one which I agree with for certain labels, and for certain people. I am fairly sure that Vaughan would also.
Sorry for the massively long response – I feel that a lot of confusion in these arguments comes from the notion that “diagnosis” means “It is biologically caused” because a lot of other medical diagnoses are biologically caused. However, this is simply not true.
Hi Tom
Thank you for your comments. It’s clear from what you (and others) say that there is a lot of disagreement about what ‘diagnosis’ actually means. In my view, this is the crux of the issue. However you seem to very sure about what it means. You state for example that diagnosis is just “the name for a thing”. Well what sort of “thing” is it a name for?? This is quite an important question, but you rather gloss over it. You say that diagnoses refer to clusters of symptoms, but again you gloss over the question of how we decide that symptoms are actually clustered together into meaningful entities. It isn’t as straightforward as you seem to think. There is actually a lot of literature on the question of how natural kinds in science are to be understood. One prominent view in philosophy of science is that such clusters of properties or symptoms need to be causally linked in order to constitute a natural kind. This is the case whether we are talking about kinds of biological species or kinds of diseases. There is too much literature on this subject to summarise here, but one thing that comes out of it is that the issue of causation always arises somehow in relation to deciding whether or not symptom clusters are significant and valid. This is all rather general of course, but the point is that simply referring to clusters of symptoms leaves key questions unresolved.
To be more specific, and sticking for the moment with my view that diagnoses have explanatory value, I should add that I didn’t fully explain my view on the explanatory significance of diagnoses. Strictly speaking, diagnoses are not explanatory in themselves, but their explanatory value is understood within the background context of known theoretical processes and mechanisms – e.g. biochemical, histological, etc. It might be better to say that they *indicate* an explanation, rather than constituting an explanation themselves.
Now I’m obviously aware that in practice not all diagnoses seem to do this or are intended to do so. But this gets us back to the question of what exactly are they naming, if not some disease entity with the ability to explain the patient’s symptoms. If they name an apparently regularly occurring syndrome which is believed to have some sort of set of enduring features of unknown cause, are we not implicitly suggesting that there may be a causal history waiting to be uncovered when we have enough information about the relevant facts? And are we really to believe that such syndromes which occur regularly and reliably have no kind of causal history that can ever be discovered?
This doesn’t deal with the point made by some people that even symptoms such as tinnitus and headaches are actually diagnoses. Unfortunately I’m at a loss as to how to respond to such strange ideas – the idea that when I have a headache, the diagnosis is “headache”! I can only presume that such people haven’t learnt the meaning of notions such as “tautology”, “triviality”, etc. Or perhaps, being a bit more charitable, they’ve made a rubbish job of explaining clearly what they do mean. Judging by other posts on this blog, some seem happy to conduct the argument entirely at the level of “I’m right, you’re wrong”. So I don’t think I need to take that any further.
To return to the key point in my last post, I was really trying to emphasise the *motivation* for maintaining that diagnoses need have no explanatory function. It’s clear to me that this is a necessary element in the argument that there is no difference in principle between medical diagnoses and psychiatric diagnoses. Therefore those who defend the current system of psychiatric diagnoses are likely to want to press this argument. In contrast, the critics of psychiatric diagnoses maintain that that there is an important difference between them. So quite a lot seems to hang on the question of whether medical diagnoses are mainly (if not in all cases) intended to have some explanatory value. What a diagnosis means and what it is expected to do are complex questions about which much has been written by philosophers of medicine, some of whom, incidentally, are qualified doctors themselves!
I would just like to say thank you to everyone for this discussion. I am finding it really useful to help me better understand the issues. It would be great if we had some way of pulling all of this, and i’m sure many other discussions on similar threads together in one online debating arena.
Dear Richard terms like headache, tinnitus etc are diagnoses as well as symptoms
Medical diagnosis are made on similarity of clinical picture (eg symptoms) or mechanisms or causes
There is substantial overlap between medical and psychiatric diagnoses for many aspects
They are not as different as u seem to think
The use of objective tests in psychiatry is hampered by lack of tests measuring higher functions in any case.
Many medical dx are not explanatory in the way u seem to mean woth causes often obscure
Richard u seem hung up on your dx must be an explanation or it’s nothing
Curiously u seem to ignore a lot of practising doctors preferring to listen to a selected few who you agree with
Dx is a label for a state with attached info that has been described before
Dx has many functions in clinical practice – giving probabilistic information on prognosis, likely symptoms and signs as well as unusual ones, co-occurring conditions, optimum treatments, complications, differential dx as well as sometimes mechanisms and causes.
Now since we know a lot more about the typical functioning of much of the body but not the mind/brain we should not be surprised for gen medical dx we often know more about mechanisms and causes than for psych dx BUT NOT ALWAYS
Now u can plow a furrow that means u can retain your belief in the primacy of explanation
Or u can listen to experts like Kendell and Jablensky who talk about utility functions of dx not just validity
Or even listen to clinicians like myself who use dx
U should also remember that even when clinicians had dx with faulty explanations eg the humoural model they were still able to obtain & use clinically useful info by careful observation
Here’s hoping u can think afresh and not just persist in your mistake
Dear Sami
You say this about my views: “Richard u seem hung up on your dx must be an explanation or it’s nothing”. What I actually said about diagnoses having an explanatory function is this: “Now I’m obviously aware that in practice not all diagnoses seem to do this or are intended to do so”. But it does seem clear to me that a large number of medical diagnoses do have a function of indicating an explanation when set against the relevant theoretical context. In saying this, I’m only reflecting a view which is widespread in the literature, even if not universally endorsed.
I’m well aware of the Kendell and Jablensky paper – I read it some time ago. I don’t dispute that psychiatric diagnoses have some utility. Indeed it’s obvious that they do – if they didn’t, they would have disappeared long ago. The issues in the debate about psychiatric diagnoses are *how* useful are they and *for whom* are they most useful. In this context, the issues of utility and validity are not completely independent of each other – if we think a particular diagnosis has poor validity, we’re bound to ask what use does it really have.
I’m glad you commented on the old humoural model. In ancient times, even medieval times, this model was the best one available. People used this to provide what they believed to be the best explanations for their somatic complaints – in this respect it did provide explanations of a sort. People do want explanations for their complaints! Obviously the progress of modern science from the 17th century onwards rendered such explanatory attempts obsolete.
But your continuing insistence that explanatory functions are not what diagnoses are primarily expected to do reinforces my point that this is a central issue in the debate about whether or not psychiatric diagnoses are different in important respects from medical ones. Indeed, this is the point I’ve been making all along.
“On a personal basis, I’m happy for people to use whatever framework they find useful to understand their own experiences.” Me too, but often the person is not given the space or time to describe their experience or its not attended to in a trauma-informed care approach. I hope the time is coming where people can describe their different experience safely and be responded to safely.
Hi Mindhacks
Has anyone done a critique of Ezra Pound’s diagnosis?
Fantastic blog post Vaughan! I’ve provided a bit of an extension of the discussion of biological markers for mental illness here: http://eiko-fried.com/all-mental-disorders-are-brain-disorders-not/
What I didn’t have space to address in the blog post is reliability. You argued that reliability in structured interviews is much higher, and cite http://journals.sagepub.com/doi/10.1177/1073191116638410 with much higher kappa values (0.72 for MDD).
Two brief replies. First, n=121 is not sufficient evidence to convince me, although I don’t doubt that structured clinical interviews leads to somewhat increased reliability. Is there more work on the topic?
Second, and more importantly, I would argue that over 99% of all studies in the literature (including, but not limited to: sociology, clinical psychology, many other fields of psychology that often assess depression as a covariate, psychiatry, and epidemiology) have used rating scales in the last decades, and not structured interviews, to assess depression severity or putative depression diagnosis. This is obvious when looking at the citations, where 3 rating scales for MDD (BDI, HRSD, CES-D) are among the top 100 cited papers in all of science, ever (https://www.nature.com/news/the-top-100-papers-1.16224). So while structured interviews might have higher and even acceptable reliability coefficients, this is not the way mental disorders are commonly measured in scientific studies.
Unrelated, I also wanted to briefly mention Pluto here, which adds yet another argument to your list stating that psychiatry isn’t really doing worse in terms of social norms influencing categories. Ken describes this in detail in his recent fantastic paper https://www.ncbi.nlm.nih.gov/pubmed/26833596: biological taxonomy is highly contentious (and would look different if you repeated the world a few times), and the heated discussions within the International Astronomical Union about down-grading Pluto to a ‘dwarf planet’ resembled modern nosological debates in psychiatry.
Best wishes
Eiko
I am very happy that there is someone around who expresses a critical thought towards the psychiatric diagnosis, and that he does to an audience of clinical psychologists. It is very difficult to talk about alternative diagnostic methods or to understand the statistical nature of the various diagnostic manuals and the definitions contained in them, not to be understood as concrete entities but as “mathematical” phenomena.