 A couple of online articles have discussed whether you would be conscious of being shot in the head with the general conclusion that it is unlikely because the damage happens faster than the brain can register a conscious sensation.
A couple of online articles have discussed whether you would be conscious of being shot in the head with the general conclusion that it is unlikely because the damage happens faster than the brain can register a conscious sensation.
While this may be true in some instances it ignores that fact that there are many ways of taking a bullet to the head.
This is studied by a field called wound ballistics and, unsurprisingly when you think about it, the wound ballistics of the head are somewhat special.
Firstly, if you get shot in the head, in this day and age, you have, on average, about a 50/50 chance of surviving. In other words, it’s important to note that not everyone dies from their injuries.
But it’s also important to note that not every bullet wound will necessarily damage brain areas essential for consciousness.
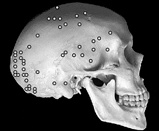
The image on the top left of this post charts the position of fatal gunshot wounds recorded in soldiers and was published in a recent study on combat fatalities.
For many reasons, including body armour and confrontation type, head wounds to soldiers are not necessary a good guide to how these will pan out in civilians, but you can see that there are many possibilities with regard to which brain areas could be affected.
In fact, you can see differences in the effect of gunshots to the head more directly from the data from Glasgow Coma Scale (GCS) ratings. A sizeable minority are conscious when they first see someone from the trauma team.
It’s also worth noting that deaths are not necessarily due to brain damage per se, blood loss is also a key factor.
An average male has about 6 litres of blood and his internal carotid artery clears about a quarter of a litre per minute at rest to supply the brain. When in a stressful situation, like, for example, being shot, that output can double.
If we need to lose about 20% of our blood to lose consciousness, our notional male could black out in just over two minutes just through having damage to his carotid. However, that’s two minutes of waiting if he’s not been knocked unconscious by the impact.
But if we’re thinking about brain damage, the extent depends on a whole range of ballistic factors – the velocity, shape, size and make-up of the bullet being key.
As it turns out, the brain needs special consideration, not least because it is encased in the skull.
One of the first things to consider is that the skull can fracture and how the fragments themselves can become missiles. In 42 cases of civilian gunshot wounds to the brain two neurosurgeons were able to find bone chips in 16 patients’ brains simply by “digital palpation” – which is a complicated medical term for sticking your fingers in and wiggling them about.
In other words, a shot to one part of the head may have knock-on effects purely due to skull shattering.
However, the skull also sets up a unique target due to its enclosed nature. If someone gets shot in the leg the pressure of the impact can be released into the surroundings. If a bullet gets into the brain the options are fewer because the pressure waves and, indeed, the brain, are largely trapped inside a solid box of bone.
If you want to get an idea of the sorts of pressures involved, just catch a video or two of bullets being fired into ballistic gel and think what would happen if the gel was trapped inside a personally important life-sustaining box.
In fact, if the shot is powerful enough, from high velocity rifles for example, there is a combination of the initial impact and an ‘explosive’ effect which can do substantial damage through forcing the brain to the side of the skull and fracturing from the inside out.
There is one rare effect, called the Krönlein shot, where a high powered shot messily opens the skull but neatly ejects the whole brain on the ground. You can find pictures on the web from pathology articles but, I warn you, they’re neither child friendly nor particularly good tea-time viewing.
Small low-velocity rounds can do quite local damage, however, and despite the tragedy of being shot, we have learnt a surprising amount from people who have survived such wounds.
As we’ve discussed previously, the use of small bore low-velocity bullets during World War I meant that more than ever before and, perhaps since, soldiers survived with small localised brain injuries.
This meant doctors could do some of the first systematic studies into how specific brain areas related to specific functions, based on tests of what brain-injured soldiers could no longer do.
But while it’s true to say that many people will lose consciousness before they even know they’ve been shot, it’s not guaranteed. Although it will mean that some people will be unfortunately aware of their death, it also means that others are able to save themselves.
 Today’s New York Times has a huge feature on the illicit use of stimulant drugs like Ritalin and pharmaceutical amphetamines in colleges and schools by kids ‘seeking an academic edge’.
Today’s New York Times has a huge feature on the illicit use of stimulant drugs like Ritalin and pharmaceutical amphetamines in colleges and schools by kids ‘seeking an academic edge’. A curiously recursive case of psychosis,
A curiously recursive case of psychosis, 
 The latest
The latest 





 A fantastic
A fantastic  A
A 


