
Life-sized edible brain sculptures from a series called ‘What have you got in your head?’ by artist Sara Asnaghi.
Life-sized edible brain sculptures from a series called ‘What have you got in your head?’ by artist Sara Asnaghi.
 I’ve just stumbled across a special issue of Neurosurgical Focus on deliberate skull deformations that tracks the practice of molding the shape of the skull from ancient times to the modern body modification scene.
I’ve just stumbled across a special issue of Neurosurgical Focus on deliberate skull deformations that tracks the practice of molding the shape of the skull from ancient times to the modern body modification scene.
All of the articles are free to access but I recommend the pieces on the politics of head deformation and the practice in the ancient Mayan and Proto-Bulgarian cultures.
But perhaps the most surprising article is on modern deliberate skull deformities in adults that covers the body modification scene (drilled in metal mohawk anyone?) and the modern trepanation movement who advocate drilling a hole in the head to achieve an altered state of consciousness.
The trepanation section has the completely fascinating and somewhat oddball history of its modern revival.
The history of the International Trepanation Advocacy Group can be traced back to a Dutch medical student and admitted polysubstance abuser named Bart Huges, who was ultimately denied his medical degree by the University of Amsterdam at least in part for his vocal advocacy of marijuana use. During one particular episode in the early 1960s while under the influence of recreational psychoactive drugs, Huges came to believe that drilling a hole in one’s head would allow blood to more freely pulse around the brain, reproducing the state of an infant’s brain prior to closure of the cranial sutures. He was aware that by adulthood, the brain is denied an elastic bony covering against which to expand; in addition, he proposed that gravity gradually robbed the brain of some of its blood volume.
Trepanation, as his theory went, had the potential to reverse both of these processes. Huges felt that prolonged standing on one’s head could yield the same result, albeit temporarily, but only with trepanation could a long-term so-called “permanent high” be attained. He eventually delineated his ideas in a 1962 monograph alternately entitled either Homo Sapiens Correctus, named for what he believed would describe a new species of humans with holes in their skulls, or The Mechanism of Brainbloodvolume (BBV). He later also authored the book, Trepanation: the Cure for Psychosis, and an autobiography, The Book With the Hole. Although never finishing medical school, he did in 1965 successfully self-trepan, and, based on what he felt was an excellent benefit from this procedure, later convinced others to do the same.
It only gets weirder from there on in.
Highly recommended (the article, not drilling holes in your head).
Link to Neurosurgical Focus on skull deformations.
Link to article on ‘Modern induced skull deformity in adults’.
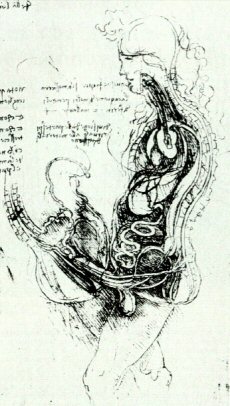 In Leonardo da Vinci’s anatomical drawings, the penis is connected directly to the brain.
In Leonardo da Vinci’s anatomical drawings, the penis is connected directly to the brain.
A 1986 article “On the sexual intercourse drawings of Leonardo da Vinci” explains why this connection, still commonly proposed today (although mostly as a metaphor it must be said), was thought to be anatomical fact by the great master.
“A brief glance at the male character in Fig. 3 reveals the amazing internal ‘plumbing’ designed by Leonardo to describe Aristotelian physiology. He has drawn two canals in the penis, the lower of which is connected to the urogenital tract via the urethra, while the upper canal passes to the spinal cord by means of three vessels. The close-up of the penis demonstrates these two canals in fine detail. In ancient Greek writing, the ‘essence’ of a baby was provided by the ‘universal seed stuff’ of the male. This procreative ingredient was derived from animal spirit, a physiological material necessary for muscular activity. The animal spirit was manufactured from arterial blood at the base of the brain and was transferred to all parts of the body through the nerves. Hence da Vinci’s spinal connection to the penis.”
And before I hear a “Yeah, right on Leo!” from the ladies, I note a remarkably similar vagina – spinal cord connection also makes an appearance in the diagram.
 The Daily Mail is a UK newspaper famous for a moralising obsession with teen sex and a tragic, long-term science impairment.
The Daily Mail is a UK newspaper famous for a moralising obsession with teen sex and a tragic, long-term science impairment.
Most of their science stories are simply face-palm material but occasionally they produce unintentional works of comic genius.
Today, is one of those days.
Teenage sex ‘leads to bad moods’ in later life’
Having sex during teenage years could lead to bad moods, changes in brain development and smaller reproductive tissues, according to scientists.
Researchers from Ohio State University College of Medicine found that these changes can occur because the sexual experience is taking place while the brain is still developing.
Study co-author John Morris said: ‘Having a sexual experience during this time point, early in life, is not without consequence.’
The researchers based their conclusions after studying the behaviour of hamsters after they engaged in sexual activity.
 The New York Times has a fascinating article about how brain damaged people in the ‘minimally responsive state’ can become more alert, curiously, after being given a type of sleeping pill.
The New York Times has a fascinating article about how brain damaged people in the ‘minimally responsive state’ can become more alert, curiously, after being given a type of sleeping pill.
The drug is called zolpidem and occasional case reports of it increasing alertness in poorly responsive neurological patients have been kicking around for some years. We reported on an early case back in 2006.
It must be said that there is still very research little in this area – some scattered case studies and a trial that recruited just three children, so I’m not sure about the wisdom of the ‘A Drug That Wakes the Near Dead’ headline.
However, the article reports on ongoing research and has a video showing the marked effect on one patient diagnosed with ‘minimally conscious state’ or MCS.
This year, scientists at Moss Rehabilitation Research Institute and at the University of Pennsylvania, both in the Philadelphia area, began the first large-scale clinical study of zolpidem as a treatment for disorders of consciousness. (Amantadine, a drug used to treat Parkinson’s disease, and the anti-anxiety medication Ativan also show promise in increasing awareness in minimally conscious patients.) So far, the evidence suggests that less than 10 percent of brain-injured patients will experience the drug’s paradoxical effects, and that among those, only a few will respond as profoundly as Viljoen did. For families like the Coxes, such odds provide a tortured kind of hope. For doctors, they bring questions. Why does a sleeping pill induce awareness in some patients but not others? And what can these bizarre awakenings tell us about the brain’s ability to heal?
A fascinating article on a curious, if limited, effect. Don’t miss the video.
Link to NYT article on zolpidem and brain injury.
 This is a video of people dancing with a recently deceased baby and it tells us something profound about the psychology of grief and mourning.
This is a video of people dancing with a recently deceased baby and it tells us something profound about the psychology of grief and mourning.
Despite a common stereotype, death of a loved one can provoke some of the most culturally diverse forms of emotion and social ritual.
The video is rare footage of the Chigualo ceremony, a mourning ritual for children aged less than seven-years-old who have just passed away from the Afrocolombian community of the Pacific coast of Colombia.
Unfortunately, there is almost nothing written about the ceremony available online in English but the Spanish language Wikipedia has good page about it.
The belief behind the ceremony is that when young children die they become angels and go straight to heaven. Therefore, these deaths are not an occasion for sadness, as many might assume, but a cause for a goodbye celebration.
You can see in the video that the Chigualo involves upbeat rhythms, singing, games and dancing – including passing the dead baby between people at the ceremony.
This may seem shocking or disrespectful to people accustomed to sadness and distress-based mourning, but in its own community it is the single most respectful way of saying goodbye to a recently blessed angel.
Psychology has a stereotype problem with grief and mourning. Over and over again false assumptions are repeated, not even valid in Western cultures, that there are certain ‘stages’ to grief, that people will reliably react in certain ways with certain key emotions – sadness, anger, resignation and so on.
This leads to both a professional pathologising of grieving people including endless variations on ‘the person hasn’t accepted their loss’, ‘they haven’t elaborated their grief’ and ‘they’re in denial’ applied to anyone who doesn’t mourn within the expected boundaries.
Moreover, it leads to a cultural blindness about how other societies feel and understand the loss of others with the implicit assumption that the experience of grief is somehow universal.
Any other reaction except extended sadness is considered to be a way of ‘masking’ supposedly inevitable pain. ‘Underneath’, it is assumed, everyone must feel the same as ‘us’.
This is despite the fact that we have a huge array of anthropological work on the vast variation in grief and mourning throughout the world.
The Akan have elaborate rituals that punctuate the year to keep the memory of dead alive. The Achuar prohibit any attempts to remember or memoralise the deceased.
The Ganda prohibit sexual activity during mourning, the Cubeo have sexual activity as part of the mourning ceremony.
A Dogon funeral is designed to ensure that spirits of the dead leave the community, an Igbo funeral that they stay.
Although death is perhaps the only experience guaranteed to be universal, our reaction to it is one of the most diverse. Consequently, respect comes in many forms.
Link to video of Chigualo ceremony.
